
The aortic valve is located between the heart and the main artery (aorta) that carries blood away from the heart. When the heart contracts, blood flows through the valve—which opens in one direction—into the aorta. The valve then closes, preventing blood from flowing back into the heart.
- It is the calcification of the valve leaflets, making it difficult for them to open. This condition is typically associated with older age. While the aortic valve normally has three leaflets, some individuals are born with only two. These individuals are predisposed to developing aortic stenosis.
- Normally, when fully open, the valve has an opening area of 2–4 cm². When this area falls below 1 cm², the stenosis is considered severe.
- Symptoms include chest pain, shortness of breath (due to heart failure), and fainting. In advanced stages of aortic stenosis, there is a risk of sudden death.
- The valve leaflets fail to come together properly, allowing blood to leak back from the aorta into the heart. As the heart becomes overloaded with volume, it leads to symptoms such as shortness of breath.
- It is often a silent condition that does not present symptoms and is usually discovered incidentally during an echocardiogram.
- In cases of ballooning of the aorta (ascending aortic aneurysm), the valve leaflets are pulled apart, resulting in regurgitation.
- If the cause of the valve regurgitation is an ascending aortic aneurysm, the aorta can be replaced with a synthetic graft using a special technique, thereby eliminating the leak.
- In cases of valve regurgitation, the leak may be repaired, but this surgery is generally not as successful or long-lasting as mitral valve repair. Valve replacement is usually necessary.
- In aortic stenosis, the aortic valve is removed and replaced with a prosthetic valve.
What Kind of Valve?
-
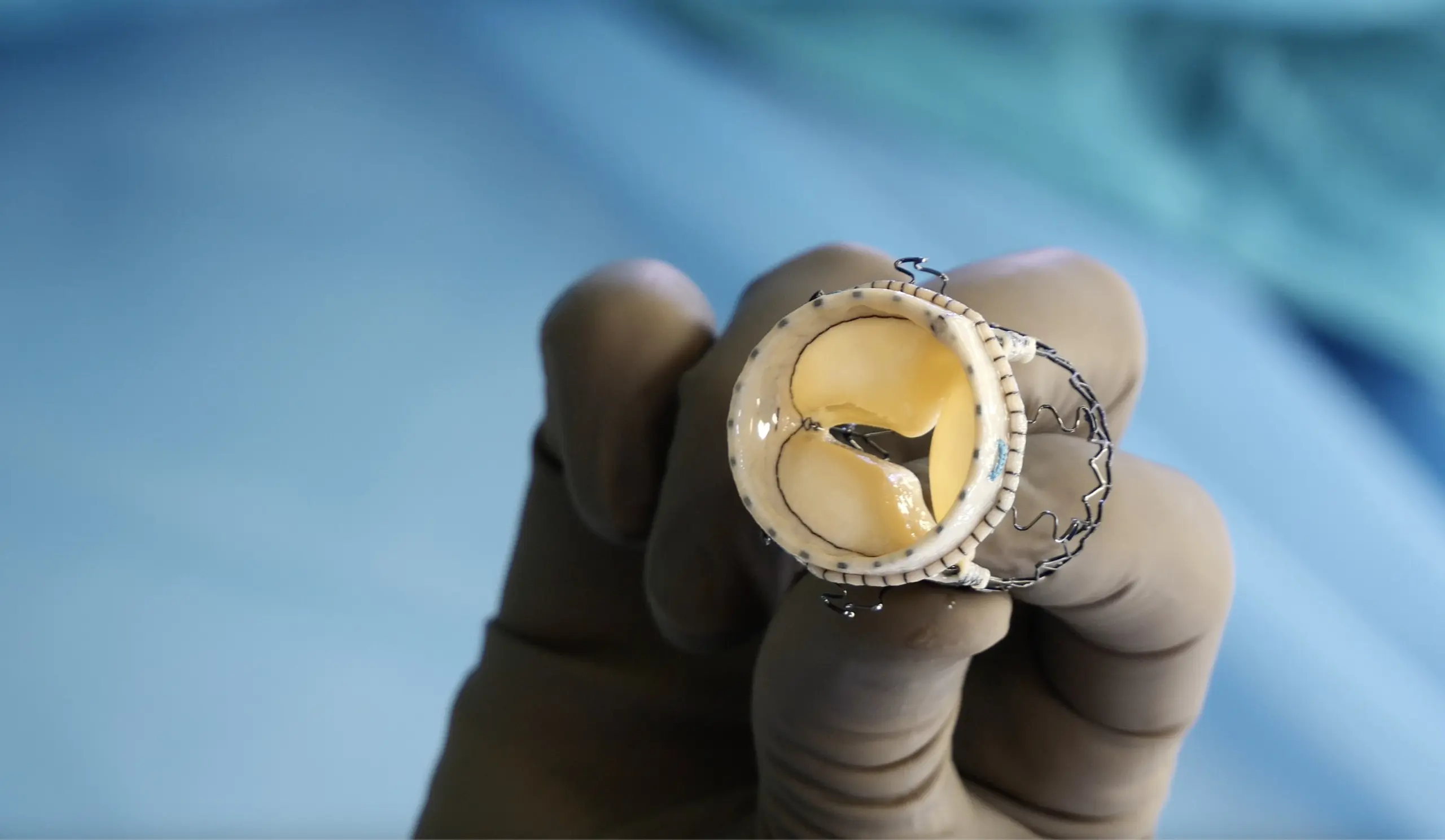
There Are Two Types of Valves: Mechanical Aortic Valve and Biological Aortic Valve
Mechanical (metal) valve: Made from titanium, it can last a lifetime without deterioration after surgery. Since it is a foreign material in the body, lifelong use of blood-thinning medication is required to prevent clot formation on the valve.Biological valve: These are tissue valves made from bovine pericardium that has been technologically decellularized. When used in patients under the age of 60–65, they may structurally deteriorate within 10–15 years, possibly requiring a second surgery. However, because they are tissue-based, they do not require long-term anticoagulant therapy.
- Göğüs kemiği kısmen açılarak, önden 5-6cm’lik bir kesiyle yapılır.
- Sağ göğüs boşluğundan dört santimetrelik bir kesiyle, kaburgaların arasından kapak değişimini yapmaktır (Right Anterior Thoracotomy _ RAT Surgery).
- İyileşme daha hızlıdır. Kozmetik olarak daha üstündür.
- A biological prosthetic valve is placed inside the narrowed valve via the groin using an angiographic technique, without any incision in the chest.
- The recovery process is very rapid, and there are no surgical scars.
- Compared to open-heart surgery, it carries higher risks (such as stroke and the need for a permanent pacemaker) and has less favorable long-term outcomes. Therefore, it is typically reserved for patients who are too high-risk to undergo conventional surgery.
-
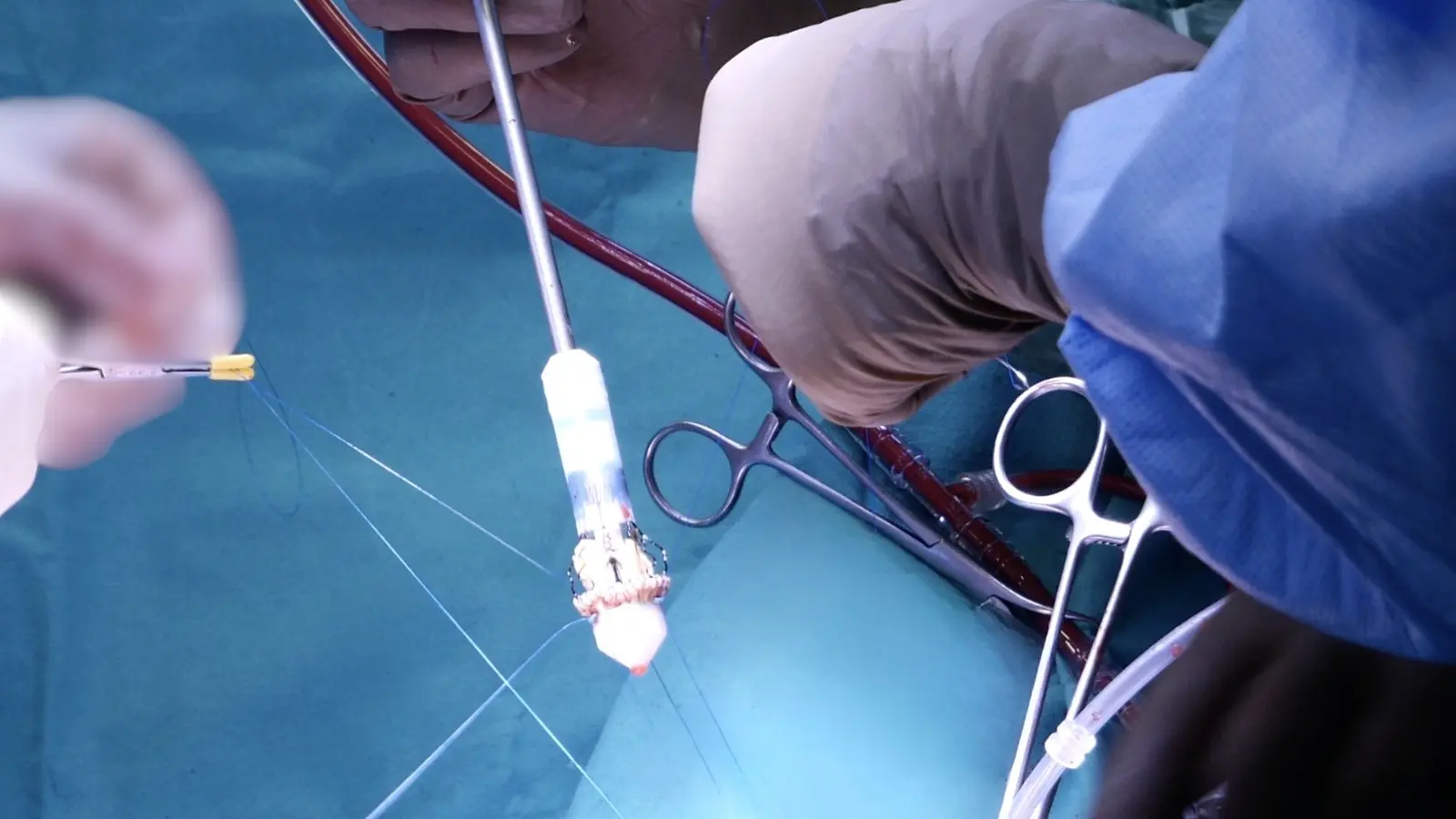
These are biological valves produced using the same technology as TAVI. After the calcified valve is removed, the new valve is positioned in place using a special deployment mechanism, without the need for individual stitches to secure it to the heart. This allows the surgery to be performed more quickly.
-
It promotes faster recovery, especially in minimally invasive surgeries. This type of procedure serves as a treatment option between TAVI and conventional open-heart surgery.
The gold standard for long-term durability of the aortic valve is surgical replacement. This involves replacing the valve through a 4-centimeter incision between the ribs on the right side of the chest (Right Anterior Thoracotomy – RAT Surgery). With advancements in technology, sutureless aortic valves have been developed, which further reduce the duration of the surgery.
- Your doctor should explain your condition to you as if you are hearing about it for the first time, with complete clarity.
- They should discuss all available treatment options—both surgical and non-surgical—along with their outcomes.
- If surgery is being considered, the doctor should explain the different approaches and recommend the one most suitable for you (such as valve repair or replacement, mechanical or biological prosthetic valves).
- They should also walk you through the entire process and associated risks, starting from the preoperative stage.
- Typically, a one-day hospital stay is required before the day of surgery to complete routine preoperative tests. These tests are performed to identify and mitigate any potential risks during surgery (such as detailed blood tests, echocardiography, carotid artery ultrasound, chest X-ray or CT scan, and pulmonary function tests).
- If you are taking blood-thinning medications, you will need to stop them 5–7 days before surgery (with the exception of Aspirin, which does not need to be discontinued). Your doctor will adjust your other medications accordingly.
- Full body shaving will be done by hospital staff (do not do it yourself; trained personnel will perform it using specialized equipment based on the planned procedure). Your nurse will explain how to bathe using a special antiseptic soap.
- If your doctor deems it appropriate, a sedative may be given the night before surgery to ensure a good night’s sleep.
- As you are taken to the operating room, you will be conscious, but due to an intravenous medication, you will not remember entering the OR.
- Heart surgeries are performed under general anesthesia. The anesthesia process itself takes approximately 45–50 minutes before the surgery begins.
- Electrodes are placed on your back to monitor your heart rhythm during the procedure. A small IV line is inserted into your arm. A special arterial cannula is placed in your wrist to continuously monitor your blood pressure throughout the surgery and intensive care stay. These steps are painless and will not be remembered due to the sedative injection administered before entering the operating room.
- General anesthesia is induced through intravenous medications. Once full anesthesia is achieved, a breathing tube is inserted into your windpipe, and your breathing is maintained with a ventilator.
- A larger IV line is placed in your neck to administer medications and fluids during and after surgery—this line also allows for blood sampling without repeated needle sticks. A urinary catheter is also inserted.
- To assess the heart during surgery—especially to evaluate valve function after valve procedures—a special probe is inserted into your esophagus to perform echocardiography.
- Your body is positioned appropriately for surgery, and the surgical area is cleaned with special antiseptic solutions.
- The surgery begins… From this moment, two additional surgeons assist your primary surgeon. One nurse dressed in sterile attire and another standby nurse are present in the room. An anesthesiologist and a technician remain at your side at all times. Two perfusionists operate the heart-lung machine, which takes over the function of your heart and lungs during the procedure.
- After the surgery is completed, you will be transferred to the intensive care unit while still under anesthesia and connected to a ventilator.
- You will not wake up in the operating room. Depending on your overall condition, you will be gradually, safely, and comfortably awakened in the ICU approximately 4–6 hours after the surgery (sometimes later).
- You will not feel any pain. Pain management medications will have been started as anesthesia is being withdrawn, and their doses will be carefully adjusted and monitored by the intensive care physician.
- One of the most common complaints in the ICU is thirst. Your fluid balance will be carefully maintained with intravenous fluids. However, since you are just waking from anesthesia, you will not be allowed to drink water freely—some patience will be needed.
- In a routine postoperative course, you will be transferred to your room in the ward around the 24th hour after surgery (this duration may be extended depending on your condition).
- Once you are transferred to your room, you will be able to take care of your personal hygiene and walk around. Bed rest is not required; in fact, it is encouraged for you to sit up and perform breathing exercises.
- You will be allowed to take a full-body shower on the 5th day.
- During your 5-day hospital stay, you will be monitored through specific blood and radiological tests.
- When it’s time for discharge, your medications will be explained to you along with a schedule showing the exact times you need to take them.
- Do not try to recreate a hospital-like environment at home. Wake up at your usual time in the morning and take frequent walks inside the house. You may receive visitors, but avoid contact with anyone who is sick to prevent infection.
- Start with short and slow outdoor walks. Gradually increase your walking distance and pace each day to build up your endurance.
- You may resume sexual activity starting from the first week after surgery.
- You will have an outpatient follow-up appointment one week after discharge. During this visit, your surgical site and medication regimen will be reviewed. After one week of regular walking, you may be ready to return to work by the third week.

